PLASMODIUM SPECIES
Plasmodium

Plasmodium species (Haemoparasite protozoa
The geographical
distribution of Plasmodium
Phylum Apicomplexa, Subphylum. Order Haemosporida, Family Plasmodiidae, Genus Plasmodium and species P. falciparum, malariae, vivax, and ovale.
Common
species of Plasmodium affecting humans
·
Plasmodium falciparum – cause malignant
tertian or sub tertian
·
Plasmodium ovale – cause ovale malaria,
Benign tertian malaria
·
Plasmodium vivax – cause vivax malaria
benign tertian malaria, mild
·
Plasmodium malariae – cause malariae
quartan malaria
Geographical
distribution
Malaria is wide spread disease
throughout the tropics and occurs also in many subtropical countries and parts
of temperature regions.
Malaria believed to be responsible for
10 -15% of death in children below 5 years of age (in Africa South of Sahara
and may invade other age groups.
·
Plasmodium vivax has a cosmopolitan distribution
it is a wide spread in tropics and subtropics
·
The species is well adapted to
temperature conditions
·
It still occurs rarely as far north as
Siberia far South Argentina and South Africa.
·
Plasmodium malariae – has a wide spread
distribution in warm countries and common in many parts of Africa, South
America, India and Malaysia.
·
Plasmodium ovale: Is a rarest of all
species and appear to be confined mainly in tropical countries particularly
West Africa.
·
Plasmodium
falciparum: Has a cosmopolitan distribution but it is a common
in tropics and subtropics
Habitats:
In man:The habitats of the parasites occur in two hosts.
In man thee parasites live in the red blood cells and
liver cell (paranchymal cells) during asexual reproduction.
The age of red blood cells appear to affect its
invasion by particular species of the
Parasites e.g. plasmodium vivax parasites the
youngest erythrocyte and plasmodium malarial the oldest while plasmodium falciparum infects
red cells of any age.
The following are stages which are found in man.
· Trophozoite – the
growing from of the parasites in the blood of man it include the ring form and
all stage onwards except the fully growth gametocytes and cells (erythrocytes).
· Schizonts – a form, which
is in process of dividing as asexually it is called “immature” when division
has just begun and mature when division is complete and the parasites cells, is
just about to rupture
· Merozoites. The process
occurs in the liver cells and red blood cells of man
This origin of the parasites is not definitely
known.
They are probably
derived from merozoites produced by schizogony in the blood stream.
· Gametocytes:
After Schizonts of red blood cell develop results in
the formation of merozoites this stage of the parasite known as male and female
gametes.
· Schizogony – A process of a
sexual reproduction by which, the nucleus and the cytoplasm divide into many
subsidiary parts.
In mosquito:
In mosquito the parasites is found in the gut or
wall in early stage and when fully developed they are found in salivary glands
of mosquito.
·
Gametes: the
male or microgametes and the female gametes or microgametes before the fertilization has taken place.
·
Zygote The
fertilized macrogamete
·
O 0o0 kinete: A zygote capable
of moving results on development/developed zygote.
·
Oocyst:An O
O kinete which has settled down become rounded and covered with membranous
cysts wall
·
Sporogony
process or cycle of sexual reproduction by which result in the formation of
sporozoites. This process occurs in the mosquito
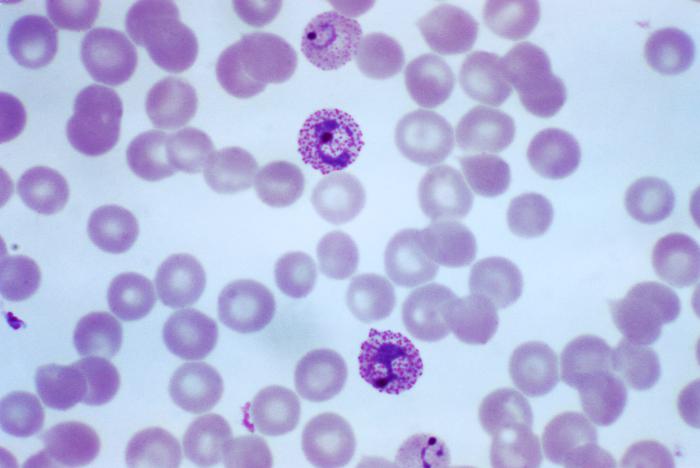
Morphological features Plasmodium
falciparum
The
diagnostic morphological features of the human plasmodia are seen in blood
smears stained by Giemsa or Field stains.
- The
earliest form after invasion of the red cell is ring of bluish cytoplasm
with dot like nucleus of red chromatin.
- The
infected red blood cells are of normal size
- The
presence of more than one ring form in a cell is relatively common.
- Presence
of double chromatin dots in an infected red cell
- The
gametocyte is banana-shaped

Plasmodium
falciparum trophozoite two parasites infected one RBC
Plasmodium
falciparum schizonts

Plasmodium falciparum gametocyte which is banana-shaped
The mode of
transmission & life cycle of
Plasmodium species
- Mosquito
bite (Female Anopheles mosquito)
- Blood
transfusion
- Congenital
- Use
of contaminated syringe as in drug
addicts
Having two stages in their life cycle.
Schizogony
or intrinsic cycle (asexual) inside human host
·
When an infected female
mosquito bites an individual it introduces sporozoites (which are contained in
its saliva) into either general blood circulation or lymphatics.
·
Within 30 minutes the
sporozoites enter the liver (parenchyma cells where they grow and multiply by
schizogony (pre-erythrocyte cycle or schizogony) leading to the production of
large Schizonts which contain many merozoites.
·
Following maturation of
Schizonts ruptured liberate merozoites
·
These young parasites
(merozoites) may re-enter or invade other cells in the case of plasmodium
ovale, plasmodium vivax and plasmodium malariae (especially old cells).
·
But this does not occur within
plasmodium falciparum so, the one which are released into the blood will invade
red blood cells to start the erythrocyte cycle (schizogony).
The
cycle in the liver (exo- erythrocytic) takes:
·
8 days with plasmodium vivax
·
5 days with plasmodium
falciparum
·
9 days with plasmodium ovale
·
11 – 12 days with plasmodium
malariae
When
merozoites invades red blood cells and start to feed cells it is called Trophozoites.
·
The trophozoites will then grow and
multiply by schizogony leading to the production of Schizonts in the red cells.
·
Following maturation the red cells
rupture releasing the Schizoints which also rupture to liberate the merozoites
which then re – invade other blood cells
·
This process will continue repeatedly
and it is here where we feel the malaria paroxysm.
·
The red cells cycle take 48 hrs with
plasmodium falciparum, plasmodium vivax, plasmodium ovale and 72 hrs with
plasmodium malariae
·
By mechanisms, which not known the
merozoite that invade cells instead of growing and multiplying, they transform
into female and male gametocytes.
·
Therefore, when another mosquito bites
man it sucks blood with gametocytes.
Sporogony or
extrinsic cycle (sexual cycle) outside the man
- When mosquito feed on man who is
infected with (malaria) or harbouring the gametocytes it is sucks blood
with female and male gametocytes.
- As the gametocytes are taken with
the blood to the gut of the mosquito the female gametocyte develops to
female gametes while the male gametocytes undergo a process of exflagellation i.e. forming
flagella like process around themselves (6- 8 in number) these are male
gametocyte.
- They detach from the parent cells
and each will then fertilize the female to form a zygote.
- In the course of growth, the zygote
elongates to form a worm like creature capable of moving called O o kinete.
- This then will move forward to the
gut wall penetrate it and come to lie on the surface to form an Oocyst.
- Following maturation, the O o cyst
will contain many sporozoites.
- This will rupture to liberate
sporozoites, which then be distributed into entire body cavity of the fly
(haemacoele).
- The sporozoites, which reach the
salivary glands, are the one, which are infective to man.

The diseases caused by Plasmodium
Malaria: The word in
Italia means bad air (mal and aria) and it also known as paludism from a Latin
word palus. Malaria is probably the most important of the vector borne disease
which has three stages.
Cold
stage:
·
Characterized by vigour and headache
·
The patient feels cold and shivers the
temperature is high.
Fever stage:
·
The temperature rises to its
maximum and the headache is severe usually, there are pains of back and joint
and often vomiting and diarrhoea.
Sweating stage:
·
In which patient perspires the
temperature fall and the headache and other pains are relived until the next
rigor.
·
With p-vivax and p ovale
produces tertian cases of malaria with fever every 3rd days ie at 48 hours
intervals.
·
Plasmodium malariae cause
malaria with every fourth days ie 72 hours interval (Benign)
·
Plasmodium falciparum causes
malignant tertian the fever
·
There is spleen enlargement
nausea, diarrhoea and blockage of fine capillaries due to the clumping of red
cells and sticking on the capillaries wall.
·
Such, blocked vessels and
swell and finally rupture of the intercranial haemorrhage cause coma and
perhaps death (cerebral malaria) in very young children.
Prevention
Prevention and control recommended that malaria control should base
on an epidemiologist approach.
Human control: Avoiding mosquito bite
by: -
·
Selecting healthy sites for
houses on the top of hills, exposure to prevailing wind and away from known
mosquito breading sites where ever possible.
·
Screening windows and doors
with mosquito netting.
·
Using effective mosquito bed
nets during the biting hour of local mosquito vectors.
·
The impregnation of nets with
insecticides such as perimethrin increases the protection.
·
Wearing protective clothing
such as long trouces long skirts sarongs and garments with long sleeves.
·
Using mosquito repellents such
as oil of tronella dimethylpathalate mosquito repellent coils or smoke from
fire or from burning pyrethrum pellets
Using drugs to:
·
Treating active infection
especially in young children
·
Suppress the infection until
they die out.
·
Prevent infection by giving
drugs every week (chemophylaxis ant malarial).
Mosquito control.
Preventing the breeding sites of mosquito larvae by: -
·
Altering the habit to
discourage breeding e.g. preserving or planting vegetation where the vector
needs sunshine or cleaning vegetation where vectors need shade.
·
Flooding or flushing of
breeding sites (places)
·
Draining to remove surface
water filling in pond or pots holes drainage ditches.
·
Changing the salts contents of
the water.
·
Regularly spraying breeding
sites with oil or chemicals.
Destroying adult’s
mosquitoes by:
·
Regular spraying of all houses
with residual insecticide such DDT or Malathion as part of programme control
and providing no resistance of the mosquitoes to the insecticides.
Health education in:
·
Schools and village and
training primary health care workers how to teach malaria control measures.
Laboratory diagnosis:
·
Examination of stained thick,
blood film to detect the parasites and to examine white blood cells for pigment
from peripheral.
·
Examination of stained thin
blood film to identify the species and give an estimated the percentage of red
cells infected.
·
Examination of Buffy coat and
red cells immediately below it after centrifuging blood in a small narrow bore
tube. This can help sometimes if parasites are few.
Key points:
Trophozoite
·
The growing from of the parasites in the
blood of man it includes the ring form and all stage onwards except the fully
growth gametocytes and cells (erythrocytes).
Gametes:
·
The male or microgametes and the female
gametes or microgametes before the
fertilization has taken place.
The mode of
transmission of Plasmodium falciparum
- Mosquito
bite (Female Anopheles mosquito)
- Blood
transfusion
- Congenital
- Use
of contaminated syringe as in drug
addicts
- Human control: Avoiding mosquito
bite by: - Selecting healthy sites for houses on the top of hills,
exposure to prevailing wind and away from known mosquito breeding sites
where ever possible.
Evaluation:
·
Explain the geographical distribution of
Plasmodium species
·
Describe the mode of transmission &
life cycle of Plasmodium falciparum
in man.
·
Explain the diseases caused by Plasmodium falciparum.
References
- Brown .H.W. (1968). Basic clinical
Parasitology (3rd ed). New York: Meredith
- CDC (2009). DPDx, Laboratory
Identification of Parasites of Public Health Concern.
- Cook, G. (2000). Manson’s Tropical
Diseases (22nd ed.). London: WB Saunders
- Harwood, R.F., James, M.T., (1979).
Entomology in Human and Animal Health (7th ed.).
- Mike, S. (2004). Medical Entomology
for students. London: Oxford University Press.
- Monica, C. (1987). Medical
Laboratory Manual for Tropical Countries. Volume 1
- Monica, C. (1998). District
Laboratory Practice in Tropical Countries. Part 1. Tropical
- Monica, C. (2000). District
Laboratory Practice in Tropical Countries. Part 2. Tropical


Comments
Post a Comment